
Jun 25
HAI Outcomes, Treatment & Surveillance in Aged Care
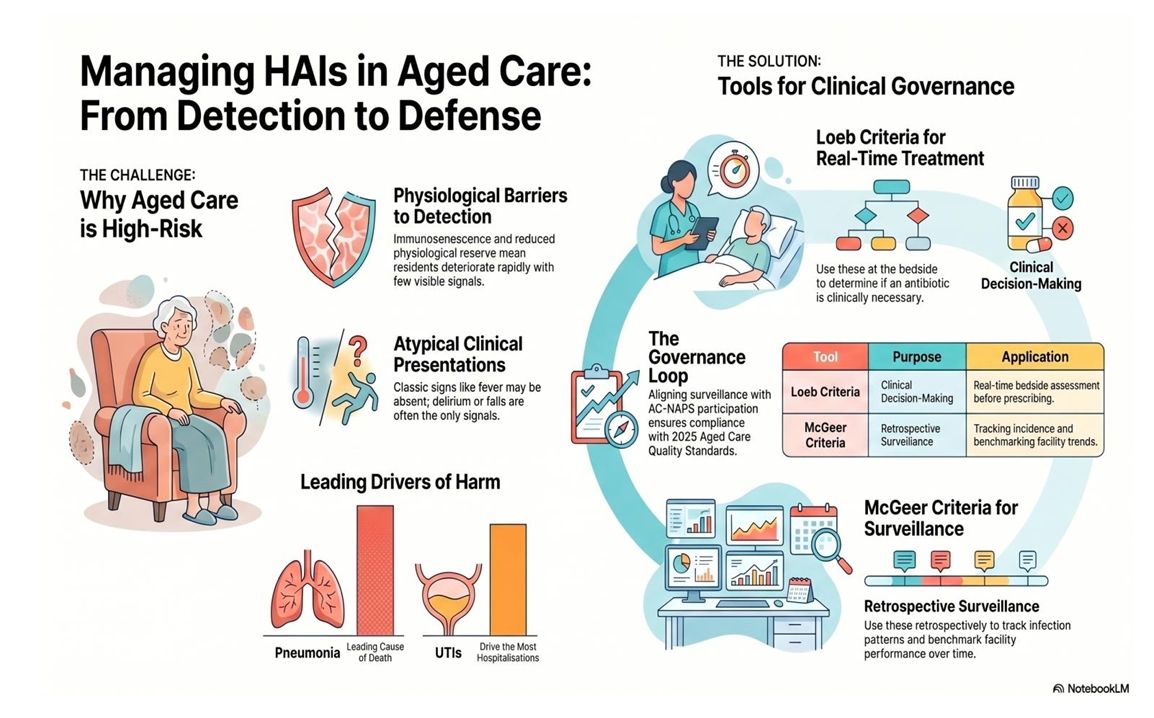
Using McGeer Criteria, Loeb Criteria & AMS to Reduce Infection Harm
In the first blog in this series, we looked at the infections your residents are most likely to encounter - urinary tract
infections (UTIs), respiratory tract infections, skin and soft tissue infections, and gastrointestinal illnesses - and how
the seasons shape their patterns. Now learn how aged care providers in Australia can reduce HAI harm through
effective surveillance using McGeer criteria, bedside decision-making with Loeb criteria, and antimicrobial
stewardship best practice.
The outcomes of healthcare-associated infections (HAIs) in aged care are serious, but they’re not inevitable. How your facility responds - through effective surveillance, sound clinical decision-making, and a genuine commitment to antimicrobial stewardship (AMS) - determines how much of that harm can be prevented.
The outcomes of healthcare-associated infections (HAIs) in aged care are serious, but they’re not inevitable. How your facility responds - through effective surveillance, sound clinical decision-making, and a genuine commitment to antimicrobial stewardship (AMS) - determines how much of that harm can be prevented.
Why are Outcomes Worse in Aged Care?
Infections pose a higher risk of serious harm for aged care residents than for younger, healthier people. This isn’t
pessimism; it’s physiology and understanding it equips your team to act faster and smarter.
Several factors compound to worsen outcomes:
Several factors compound to worsen outcomes:
- Immunosenescence blunts the immune response, meaning infections progress further before the body mounts a visible defence.
- Reduced physiological reserve leaves less capacity to compensate; a resident who appears “only a bit unwell” may be closer to clinical deterioration than their presentation suggests.
- Polypharmacy introduces drug interactions and alters pharmacokinetics, particularly in residents with renal impairment, affecting how antibiotics are absorbed, distributed, and cleared.
- Atypical presentation means classic infection signs, such as fever, focal pain, and localised symptoms, may be absent; delirium, falls, or functional decline may be the only early signal.
- Comorbidities reduce tolerance for both infection and treatment.
The result is a population in which infection spreads faster, deteriorates more rapidly, and responds more unpredictably to treatment than teams are sometimes prepared for.
What Are the Real Consequences of Common HAIs?
- Pneumonia is a leading cause of death among aged care residents. Respiratory tract infections (RTIs) have the highest HAI mortality among infection categories in this setting. Aspiration pneumonia, driven by swallowing dysfunction and poor oral hygiene, is a significant yet often overlooked contributor. A resident who aspirates regularly is not just a dysphagia management challenge; they’re at ongoing risk of infection at every meal.
- Urinary tract infections are the leading cause of infection-related hospitalisations. They also cause delirium, falls, functional decline, and, critically, antimicrobial resistance (AMR) driven by decades of inappropriate prescribing. Antimicrobial resistance rates in residential aged care are significant and, for some organisms, higher than in community and hospital settings. Up to 70% of aged care residents receive at least one course of systemic antibiotics each year. That is not a treatment statistic - it’s an overuse signal.
- Skin and soft tissue infections, if not identified early, can progress to wound breakdown, sepsis, and hospitalisation. Infected pressure injuries pose clinical and governance risks, particularly under the Strengthened Aged Care Quality Standards introduced by the Aged Care Act (2024).
- Gastrointestinal infections, particularly Clostridioides difficile (C. diff), are both a direct consequence of
antibiotic overuse and a serious clinical outcome. C. diff causes significant morbidity, recurs in a substantial
proportion of cases, and is difficult to control once it has established within a facility.

How Should Infections Be Treated in Aged Care?
Treating infections in aged care is not simply a matter of prescribing the right antibiotic. It requires clinical
judgement on whether an antibiotic is needed at all, which agent is appropriate, and the duration of treatment.
The Loeb criteria, developed by Dr Mark Loeb and colleagues and published in 2001, set the minimum clinical threshold for initiating antibiotics in aged care residents. Unlike surveillance tools, the Loeb criteria are designed for real-time bedside decision-making, often before diagnostic results are available. They exist precisely because clinicians sometimes feel pressure to “do something” before the clinical picture is clear.
For your nursing team, the practical lesson is straightforward: document specifically. “Temperature 38.2°C at 1430hrs, febrile for the second consecutive assessment, new onset of dysuria and frequency reported” gives a prescriber something to work with. “Seems a bit unwell, possible UTI” doesn’t, and that kind of documentation drives inappropriate prescribing.
The Loeb criteria, developed by Dr Mark Loeb and colleagues and published in 2001, set the minimum clinical threshold for initiating antibiotics in aged care residents. Unlike surveillance tools, the Loeb criteria are designed for real-time bedside decision-making, often before diagnostic results are available. They exist precisely because clinicians sometimes feel pressure to “do something” before the clinical picture is clear.
For your nursing team, the practical lesson is straightforward: document specifically. “Temperature 38.2°C at 1430hrs, febrile for the second consecutive assessment, new onset of dysuria and frequency reported” gives a prescriber something to work with. “Seems a bit unwell, possible UTI” doesn’t, and that kind of documentation drives inappropriate prescribing.
Treatment by infection type:
- UTIs: First-line oral options for uncomplicated lower UTI typically include nitrofurantoin or trimethoprim, guided by local resistance patterns and Therapeutic Guidelines. Treatment should start only when genuine clinical criteria are met - not based on a positive dipstick, malodorous urine, or confusion alone. Duration should be as short as the evidence supports. Delirium alone should not be assumed to indicate a urinary tract infection without supporting clinical signs. Over-reliance on this association remains a key driver of inappropriate prescribing.
- Pneumonia: Community-acquired pneumonia guidelines apply. The key decision is whether to treat in place or transfer to hospital, and this requires an honest, current advance care plan.
- C. diff: Oral vancomycin or fidaxomicin, with fidaxomicin preferred when recurrence risk is a concern. Discontinue the triggering antibiotic if clinically safe. Contact precautions are essential and non-negotiable.
- Skin and wound infections: Take a wound swab for culture when clinical signs of infection are present and
results will influence management, ideally before starting antibiotics. Systemic treatment addresses the
infection, while wound management and removal of the underlying causes - pressure, poor circulation,
moisture - prevent recurrence.
What Are the McGeer Criteria and Why Do They Matter?
Good treatment starts with good detection - and that’s where surveillance comes in.
The McGeer criteria, originally developed by Dr Allison McGeer in 1991 and significantly revised in 2012, are the internationally recognised standardised definitions of infection for long-term care settings. They were designed specifically for aged care residents - a population for whom standard hospital-based criteria don’t apply. The 2012 revision tightened the UTI and RTI definitions and added new criteria for norovirus gastroenteritis and C. diff.
It’s worth being clear about what the McGeer criteria are, and what they aren’t. They are a “retrospective surveillance tool”. They help you determine whether an HAI occurred, estimate incidence and prevalence, and benchmark your facility’s infection rates over time. They are not a real-time clinical decision tool at the bedside - that’s the role of the Loeb criteria.
The distinction matters in practice. A resident can have a genuine infection without meeting the McGeer surveillance criteria. Conversely, meeting the criteria doesn’t automatically mean an antibiotic was indicated. Using McGeer correctly means applying it consistently, documenting clearly, and using the data to identify patterns: which infections, which units, which residents, and which time of year.
For Australian facilities, participation in the Aged Care National Antimicrobial Prescribing Survey (AC-NAPS), coordinated by the National Centre for Antimicrobial Stewardship (NCAS-Australia), is one of the most effective steps your facility can take. It benchmarks your prescribing against peer facilities and provides your governing body with meaningful data to act on. New Zealand facilities should use local surveillance and audit tools and engage with regional antimicrobial stewardship initiatives where available
The McGeer criteria, originally developed by Dr Allison McGeer in 1991 and significantly revised in 2012, are the internationally recognised standardised definitions of infection for long-term care settings. They were designed specifically for aged care residents - a population for whom standard hospital-based criteria don’t apply. The 2012 revision tightened the UTI and RTI definitions and added new criteria for norovirus gastroenteritis and C. diff.
It’s worth being clear about what the McGeer criteria are, and what they aren’t. They are a “retrospective surveillance tool”. They help you determine whether an HAI occurred, estimate incidence and prevalence, and benchmark your facility’s infection rates over time. They are not a real-time clinical decision tool at the bedside - that’s the role of the Loeb criteria.
The distinction matters in practice. A resident can have a genuine infection without meeting the McGeer surveillance criteria. Conversely, meeting the criteria doesn’t automatically mean an antibiotic was indicated. Using McGeer correctly means applying it consistently, documenting clearly, and using the data to identify patterns: which infections, which units, which residents, and which time of year.
For Australian facilities, participation in the Aged Care National Antimicrobial Prescribing Survey (AC-NAPS), coordinated by the National Centre for Antimicrobial Stewardship (NCAS-Australia), is one of the most effective steps your facility can take. It benchmarks your prescribing against peer facilities and provides your governing body with meaningful data to act on. New Zealand facilities should use local surveillance and audit tools and engage with regional antimicrobial stewardship initiatives where available

How Do You Turn Surveillance Data into Better Outcomes?
Surveillance without action is just paperwork. The facilities that achieve the best HAI outcomes integrate
surveillance data into a clear governance loop: regular review by your Infection Prevention and Control (IPC) and
AMS committee, feedback to prescribers on prescribing patterns, and quality improvement projects linked to your
findings.
Under Outcome 5.2, Action 5.2.1 of the Strengthened Aged Care Quality Standards (effective 1 November 2025), providers are explicitly required to implement both an AMS system and IPC processes for clinical care — including processes to prevent, identify, and manage UTIs, and to review the use of invasive devices such as urinary catheters. The Aged Care Quality and Safety Commission (ACQSC) expects to see evidence of compliance.
The good news is that multi-component programs work. Interventions that combine education, monitoring, feedback, and at least four coordinated components consistently reduce HAI rates in residential settings. No single measure is enough — but when your team, governance structures, surveillance system, and AMS program are aligned, the difference is measurable.
Under Outcome 5.2, Action 5.2.1 of the Strengthened Aged Care Quality Standards (effective 1 November 2025), providers are explicitly required to implement both an AMS system and IPC processes for clinical care — including processes to prevent, identify, and manage UTIs, and to review the use of invasive devices such as urinary catheters. The Aged Care Quality and Safety Commission (ACQSC) expects to see evidence of compliance.
The good news is that multi-component programs work. Interventions that combine education, monitoring, feedback, and at least four coordinated components consistently reduce HAI rates in residential settings. No single measure is enough — but when your team, governance structures, surveillance system, and AMS program are aligned, the difference is measurable.
Your residents deserve nothing less.
Take-Home Message
HAIs in aged care are serious — but how your facility responds makes the difference. Use the Loeb criteria at the
bedside to guide antibiotic decision-making. Use the McGeer criteria to track infection patterns across your facility.
Join AC-NAPS. Build a governance loop that actually closes. When surveillance, AMS, and your IPC program work
together, you don’t just manage infections - you prevent them.
Sources
Loeb et al., “Development of minimum criteria for the initiation of antibiotics in residents of long-term-care facilities” (Infection Control and Hospital Epidemiology, 2001); Stone et al., “Surveillance definitions of infections in long-term care facilities: revisiting the McGeer criteria” (Infection Control and Hospital Epidemiology, 2012); Hilliard, “Antibiotic Stewardship in Long-Term Care: Leveraging McGeer and Loeb Criteria for Better Outcomes” (Infection Control Today, 2025); UTIs in residential aged care facilities (RACGP Australian Journal of General Practice, 2022); Preventing and Controlling Infections in Delivering Clinical Care Services, Outcome 5.2 (Aged Care Quality and Safety Commission, ACQSC, 2025); Root Cause Analysis to Identify Strategies to Prevent Infection-Related Hospitalisations from Australian Residential Aged Care Services (PMC, 2020).
Loeb et al., “Development of minimum criteria for the initiation of antibiotics in residents of long-term-care facilities” (Infection Control and Hospital Epidemiology, 2001); Stone et al., “Surveillance definitions of infections in long-term care facilities: revisiting the McGeer criteria” (Infection Control and Hospital Epidemiology, 2012); Hilliard, “Antibiotic Stewardship in Long-Term Care: Leveraging McGeer and Loeb Criteria for Better Outcomes” (Infection Control Today, 2025); UTIs in residential aged care facilities (RACGP Australian Journal of General Practice, 2022); Preventing and Controlling Infections in Delivering Clinical Care Services, Outcome 5.2 (Aged Care Quality and Safety Commission, ACQSC, 2025); Root Cause Analysis to Identify Strategies to Prevent Infection-Related Hospitalisations from Australian Residential Aged Care Services (PMC, 2020).
We are on Facebook and LinkedIn – Like us, follow and share
For further information on this topic, see the HUB, the IPS website. EVE, our “bot”, will answer a quick question, or email support@infectioncontrol.care if you need help.
Follow our blogs, and if there is any subject you’d like us to delve into, email our support team.
For further information on this topic, see the HUB, the IPS website. EVE, our “bot”, will answer a quick question, or email support@infectioncontrol.care if you need help.
Follow our blogs, and if there is any subject you’d like us to delve into, email our support team.

Lyndon Forrest
Managing Director | CEO
Lyndon is the Managing Director of Infection Prevention Services (IPS), bringing over 30 years' experience supporting aged care providers across Australia and New Zealand.
With a background spanning outbreak response, compliance, and infection risk management — alongside hands-on experience leading teams, managing multi-site operations, and navigating business turnaround — he understands both the clinical and organisational pressures aged care providers face. Lyndon holds a Master of Commerce (Industrial Relations), and applies that foundation to the people, process, and growth challenges that come with running a complex healthcare services business.
He is passionate about building the systems and capability that make infection prevention sustainable — not just compliant — and about helping organisations grow their confidence alongside their practice.
Lyndon's focus is straightforward: strengthen operations, develop the right people, and drive proactive infection prevention strategies that protect residents, staff, and communities for the long term.
Lyndon is the Managing Director of Infection Prevention Services (IPS), bringing over 30 years' experience supporting aged care providers across Australia and New Zealand.
With a background spanning outbreak response, compliance, and infection risk management — alongside hands-on experience leading teams, managing multi-site operations, and navigating business turnaround — he understands both the clinical and organisational pressures aged care providers face. Lyndon holds a Master of Commerce (Industrial Relations), and applies that foundation to the people, process, and growth challenges that come with running a complex healthcare services business.
He is passionate about building the systems and capability that make infection prevention sustainable — not just compliant — and about helping organisations grow their confidence alongside their practice.
Lyndon's focus is straightforward: strengthen operations, develop the right people, and drive proactive infection prevention strategies that protect residents, staff, and communities for the long term.
Erica Callaghan
Marketing Manager
Erica Callaghan is a dedicated professional with a rich background in agriculture and nutrient management. Growing up on her family's farm in Mid Canterbury, she developed a deep passion for farming. She currently resides on her partner's arable property in South Canterbury.
In 2017, Erica joined the Farm Sustainability team, focusing on nutrient management and environmental stewardship. In February 2024, she became the Manager of Marketing and Sales at Bug Control New Zealand - Infection Prevention Services, where her passion now includes improving infection prevention outcomes.
Outside of work, Erica loves cooking and traveling, often combining her culinary interests with her explorations in Italy and Vietnam. She enjoys entertaining family and friends and remains actively involved in farm activities, especially during harvest season.
Erica Callaghan is a dedicated professional with a rich background in agriculture and nutrient management. Growing up on her family's farm in Mid Canterbury, she developed a deep passion for farming. She currently resides on her partner's arable property in South Canterbury.
In 2017, Erica joined the Farm Sustainability team, focusing on nutrient management and environmental stewardship. In February 2024, she became the Manager of Marketing and Sales at Bug Control New Zealand - Infection Prevention Services, where her passion now includes improving infection prevention outcomes.
Outside of work, Erica loves cooking and traveling, often combining her culinary interests with her explorations in Italy and Vietnam. She enjoys entertaining family and friends and remains actively involved in farm activities, especially during harvest season.
Toni Sherriff
Clinical Nurse Specialist
Toni is a Registered Nurse with extensive experience in Infection Prevention and Control. Her career began as a kitchen hand and caregiver in Aged Care facilities, followed by earning a Bachelor of Nursing.
Toni has significant experience, having worked in Brisbane’s Infectious Diseases ward before returning home to New Zealand, where she continued her career as a Clinical Nurse Specialist in Infection Prevention and Control within Te Whatu Ora (Health NZ).
Toni brings her expertise and dedication to our team, which is instrumental in providing top-tier infection prevention solutions to our clients.
Toni is a Registered Nurse with extensive experience in Infection Prevention and Control. Her career began as a kitchen hand and caregiver in Aged Care facilities, followed by earning a Bachelor of Nursing.
Toni has significant experience, having worked in Brisbane’s Infectious Diseases ward before returning home to New Zealand, where she continued her career as a Clinical Nurse Specialist in Infection Prevention and Control within Te Whatu Ora (Health NZ).
Toni brings her expertise and dedication to our team, which is instrumental in providing top-tier infection prevention solutions to our clients.
Julie Hadfield
Accounts & Payroll
Julie is experienced in Accounts & Payroll Administration & after a long career in both the Financial & Local Government Sectors, is now working with our team. Julie brings her strong time management & organisational skills to our team, which is important to keep the company running in the background to enable the rest of our team to provide top notch service to all of our clients.
Julie is experienced in Accounts & Payroll Administration & after a long career in both the Financial & Local Government Sectors, is now working with our team. Julie brings her strong time management & organisational skills to our team, which is important to keep the company running in the background to enable the rest of our team to provide top notch service to all of our clients.
Andrea Murray
Content Editor
I attended Otago University in NZ and graduated as a Dental Surgeon. After 40 years in the profession, I retired in 2022. Infection prevention knowledge was part of everyday practice, dealing with sterilisation, hand hygiene, and cleaning.
Before retiring, I began doing some editing and proofreading for Bug Control as I am interested in the subject and in the English language. During the COVID-19 lockdown, I attended the ACIPC course "Introduction to Infection Prevention and Control", which increased my interest in the subject. I now work part-time as the Content Editor for the company.
I attended Otago University in NZ and graduated as a Dental Surgeon. After 40 years in the profession, I retired in 2022. Infection prevention knowledge was part of everyday practice, dealing with sterilisation, hand hygiene, and cleaning.
Before retiring, I began doing some editing and proofreading for Bug Control as I am interested in the subject and in the English language. During the COVID-19 lockdown, I attended the ACIPC course "Introduction to Infection Prevention and Control", which increased my interest in the subject. I now work part-time as the Content Editor for the company.
Personally, I lived in the UK for 10 years. My two children were born in Scotland, and now both are living in Europe, one in Amsterdam, Netherlands, and the other in Edinburgh, Scotland. I live close to Fairlie on the South Island of NZ, a beautiful part of the country, and I love being out of the city.
Princess
Customer Support
Princess began her career as a dedicated Customer Service Representative, honing her communication and problem-solving skills. She later transitioned into a Literary Specialist role, where she developed a keen eye for detail. Her journey then led her to a Sales Specialist position, where she excelled in client relations.
Now, as a Customer Support professional in Infection Prevention Services. Princess focuses on ensuring customer satisfaction, building loyalty, and enhancing the overall customer journey.
Princess began her career as a dedicated Customer Service Representative, honing her communication and problem-solving skills. She later transitioned into a Literary Specialist role, where she developed a keen eye for detail. Her journey then led her to a Sales Specialist position, where she excelled in client relations.
Now, as a Customer Support professional in Infection Prevention Services. Princess focuses on ensuring customer satisfaction, building loyalty, and enhancing the overall customer journey.
Dianne Newey
Senior Infection Prevention and Control Consultant
Dianne is a Senior Clinical Consultant at Infection Prevention Services (IPS), bringing over 35 years of nursing experience and a depth of clinical knowledge that most people would need two careers to accumulate.
Having served as Clinical Director at Royal Ryde Rehabilitation Hospital alongside a career spanning the full breadth of clinical practice, Dianne has seen it all — and more importantly, knows exactly what to do about it. She is the person in the room that everyone quietly hopes will speak first.
For more than seven years she has been a cornerstone of the IPS team, providing clinical advice, developing and reviewing policies and procedures, delivering monthly IPC webinars to IP Leads, and conducting environmental audits in aged care facilities across Australia and New Zealand. If infection prevention has a question, Dianne almost certainly has the answer — and she'll deliver it with a laugh that you'll hear from the other end of the corridor.
A true fountain of knowledge, wrapped in the kind of warmth and humour that only three decades of nursing can produce. Customers don't just trust Dianne — they look forward to hearing from her.
Dianne is a Senior Clinical Consultant at Infection Prevention Services (IPS), bringing over 35 years of nursing experience and a depth of clinical knowledge that most people would need two careers to accumulate.
Having served as Clinical Director at Royal Ryde Rehabilitation Hospital alongside a career spanning the full breadth of clinical practice, Dianne has seen it all — and more importantly, knows exactly what to do about it. She is the person in the room that everyone quietly hopes will speak first.
For more than seven years she has been a cornerstone of the IPS team, providing clinical advice, developing and reviewing policies and procedures, delivering monthly IPC webinars to IP Leads, and conducting environmental audits in aged care facilities across Australia and New Zealand. If infection prevention has a question, Dianne almost certainly has the answer — and she'll deliver it with a laugh that you'll hear from the other end of the corridor.
A true fountain of knowledge, wrapped in the kind of warmth and humour that only three decades of nursing can produce. Customers don't just trust Dianne — they look forward to hearing from her.
Caoimhe (Keva) Stewart
Clinical & Business Operations Manager
Caoimhe is the Clinical & Business Operations Manager at Infection Prevention Services (IPS), bringing a clinical background as a Registered Nurse across the UK and Australia — and an almost unsettling ability to make technology do exactly what she wants.
With experience in Occupational Health, Palliative Care, and Community Nursing, she understands the real challenges faced by healthcare teams. What she may lack in stature she more than makes up for in impact — Caoimhe is the kind of person who walks into a problem, sizes it up, and has three solutions before anyone else has finished reading the brief.
Customers love her. Not just because she delivers — though she always does — but because she genuinely cares about the outcome on the other side. She is passionate about creating seamless learning experiences and empowering organisations with the tools, knowledge, and support needed to strengthen infection prevention practices and improve care outcomes.
Small in size. Mighty in results. Completely irreplaceable.
Caoimhe is the Clinical & Business Operations Manager at Infection Prevention Services (IPS), bringing a clinical background as a Registered Nurse across the UK and Australia — and an almost unsettling ability to make technology do exactly what she wants.
With experience in Occupational Health, Palliative Care, and Community Nursing, she understands the real challenges faced by healthcare teams. What she may lack in stature she more than makes up for in impact — Caoimhe is the kind of person who walks into a problem, sizes it up, and has three solutions before anyone else has finished reading the brief.
Customers love her. Not just because she delivers — though she always does — but because she genuinely cares about the outcome on the other side. She is passionate about creating seamless learning experiences and empowering organisations with the tools, knowledge, and support needed to strengthen infection prevention practices and improve care outcomes.
Small in size. Mighty in results. Completely irreplaceable.
Bridgette Mackie
Clinical Nurse Educator
Bridgette is an experienced New Zealand Registered Nurse, qualified Healthcare Auditor, and Healthcare Educator with a strong background in clinical quality, competency assessment, and infection prevention. She has led large-scale OSCE and CAP training programmes for internationally qualified nurses, developed sector-specific educational resources, and coordinated HealthCERT audit preparation in the surgical sector.
Known for her engaging teaching style and genuine passion for supporting learners, Bridgette excels at making complex topics accessible and relevant. She blends operational leadership with a deep commitment to professional development and safe, effective practice.
Bridgette is an experienced New Zealand Registered Nurse, qualified Healthcare Auditor, and Healthcare Educator with a strong background in clinical quality, competency assessment, and infection prevention. She has led large-scale OSCE and CAP training programmes for internationally qualified nurses, developed sector-specific educational resources, and coordinated HealthCERT audit preparation in the surgical sector.
Known for her engaging teaching style and genuine passion for supporting learners, Bridgette excels at making complex topics accessible and relevant. She blends operational leadership with a deep commitment to professional development and safe, effective practice.
