
Mar 2
Managing "The Itch"
A Clinical Guide for Aged Care Professionals
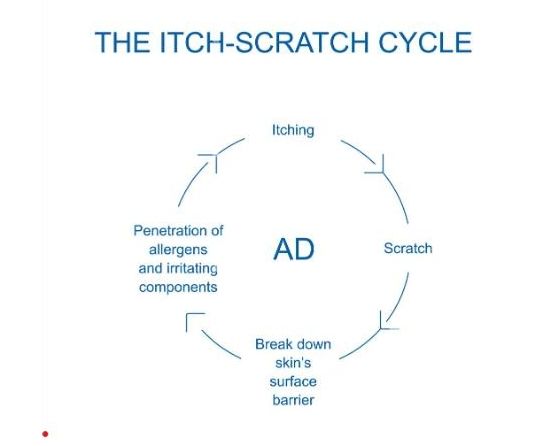
Managing pruritus (the "itch") in aged care is a daily challenge for IPC leads and clinical staff. It is not "just dry skin" - it is a puzzle where missing a single clue in the diagnosis can lead to a facility-wide outbreak or prolonged resident distress.
Itchy skin in an aged care resident can be classified into three main categories: Environmental/Structural, Infestations, and Systemic. Investigating the cause of the itch will modify treatment approaches and help identify the possibility of an outbreak.
Itchy skin in an aged care resident can be classified into three main categories: Environmental/Structural, Infestations, and Systemic. Investigating the cause of the itch will modify treatment approaches and help identify the possibility of an outbreak.

The Three Main Categories of the Itch
1. Xerosis (Dry Skin): This is the most common cause, as ageing skin produces less
sebum and retains less moisture.
- How to identify: Skin looks "crazy-paved" or flaky, usually on the shins and forearms. The itch worsens after hot showers or in low humidity, and there is no primary rash (bumps/blisters).
- Action: Implement "soap-free" washing protocols, apply thick emollients within
3 minutes of drying, and review room humidity.
2. Scabies (The IPC Priority): A parasitic infestation that requires immediate isolation
and reporting.
- How to identify: Intense itching, much worse at night. Look for small, pearly "burrows" in finger webs, wrists, or the waistline.
- Crusted Scabies: In elderly residents, look for thick, scaly plaques. These may not itch at all but contain millions of mites and are highly infectious.
- Action: Implement immediate contact precautions and treat with Permethrin 5% cream or oral Ivermectin.
3. Dermatitis (Eczema or Contact): Inflammation caused by irritants or allergies.
- How to recognise: Red, inflamed patches. Usually seen as Incontinence Associated Dermatitis (IAD) or a reaction to new laundry detergents or topical medicines.
- Action: Identify and eliminate the trigger, apply barrier creams for IAD, and use
short-term topical corticosteroids as prescribed.
Systemic and Internal Causes
When the skin appears quite normal, but the resident is persistently scratching,
consider "internal" triggers.
- Chronic Kidney Disease (CKD): Known as "Uremic itch"; skin may appear with a greyish hue. Review eGFR
- Cholestasis (Liver): Itching is often felt on the palms and soles of the feet and may be accompanied by jaundice. Check Liver Function Tests (LFTs).
- Polypharmacy: Review medications for common “itchy” side effects in culprits such as opioids, ACE inhibitors, and statins.
- Neuropathic Itch: Manifests as a burning or tingling sensation, usually localised
to a specific area such as the back.
The IPC "Red Flags"
IPC Leads should monitor for signs of a cluster to prevent a facility-wide outbreak.
- Is it spreading? If two residents in the same wing develop a new itch, treat it as Scabies until proven otherwise.
- Is it crusting? Thick scales on a resident's hands or feet are a sign of a "super spreader" event.
- Is it nocturnal? If a resident is distressed at 2:00 AM but fine during the day,
parasites are likely the main suspect.
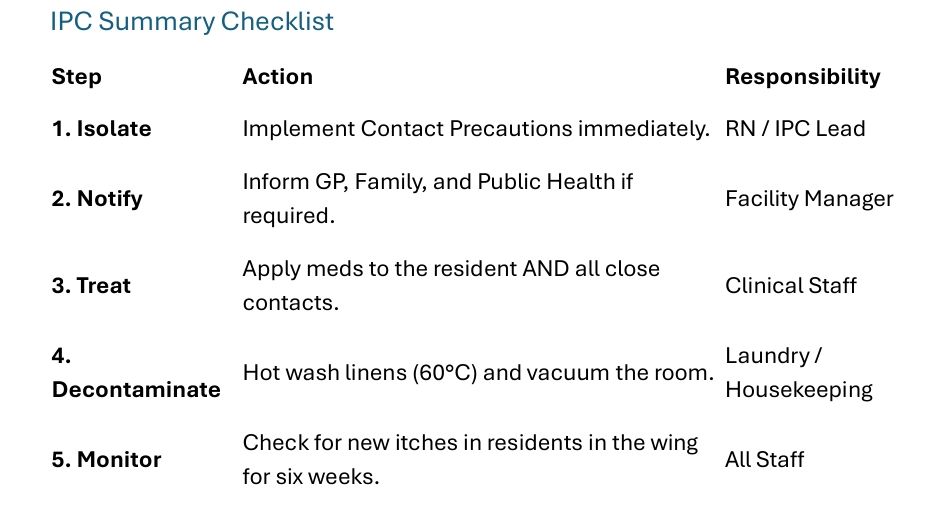
Scabies Management: The IPC "Deep Dive"
When a case is suspected, the "Scabies Protocol" must be activated immediately with a
coordinated strike.
The "Simultaneous Treatment" Rule
- Contact Tracing: Identify all staff and family members who had skin-to-skin contact with the affected resident over the past 6 weeks.
- The "Blitz": To prevent "ping-pong" infections, the index case and all close contacts (including asymptomatic roommates) must be treated simultaneously.
- Application: Topical creams must be applied from the neck down to the toes,
including under fingernails and within skin folds.

Environmental Cleaning & Laundry
Mites can survive off a human host for 48 to 72 hours.
- Linen & Clothing: All bedding and clothing used in the past 4 days must be laundered.
- Heat is the Killer: Wash at 60°C (140°F) or higher and use a hot dryer cycle for at least 20 minutes.
- Non-Washables: Seal items that cannot be washed (e.g., pillows, slippers) in a plastic bag for 7 days to starve the mites.
- Furniture: Thoroughly vacuum (a vacuum with a hepa-filter) upholstered chairs
and mattresses in the resident’s room.
Clinical Management Flowchart for Staff
- Visual Inspection: Check for burrows, rashes, or scales.
- History Check: Determine when the itching began, if it's worse at night, and if any new medications have been prescribed.
- Basic Intervention: Use a soap-free wash product and apply intensive moisturiser for 7 days.
- Escalation: If there is no improvement or a burrow is observed, notify the GP for a skin scraping or empirical treatment.
- Pro Tip: Maintain a "Skin Map" of the facility to spot geographic clusters of itchy
residents.
Conclusion
The "itch" is an essential diagnostic signal. For the HCW, it indicates the need to
moisturise and monitor; for the IPC Lead, it signals the need to investigate and contain.
By standardising our approach to these differentials, we shift from "reactive scratching"
to proactive clinical management that benefits the entire community.
See the HUB for more information from IPS.
We are on LinkedIn and Facebook – like, share and follow.
Can’t find what you’re looking for? Talk to EVE, our multilingual bot, or speak to someone real at support@infectioncontrol.care
Take advantage of our expertise in IPC. See the HUB for policies, resources and courses relating to this very important subject. Ask EVE for a quick answer to your question.
We are on LinkedIn and Facebook – like, share and follow.
Can’t find what you’re looking for? Talk to EVE, our multilingual bot, or speak to someone real at support@infectioncontrol.care
Take advantage of our expertise in IPC. See the HUB for policies, resources and courses relating to this very important subject. Ask EVE for a quick answer to your question.

Lyndon Forrest
Managing Director | CEO
Lyndon is the Managing Director of Infection Prevention Services (IPS), bringing over 30 years' experience supporting aged care providers across Australia and New Zealand.
With a background spanning outbreak response, compliance, and infection risk management — alongside hands-on experience leading teams, managing multi-site operations, and navigating business turnaround — he understands both the clinical and organisational pressures aged care providers face. Lyndon holds a Master of Commerce (Industrial Relations), and applies that foundation to the people, process, and growth challenges that come with running a complex healthcare services business.
He is passionate about building the systems and capability that make infection prevention sustainable — not just compliant — and about helping organisations grow their confidence alongside their practice.
Lyndon's focus is straightforward: strengthen operations, develop the right people, and drive proactive infection prevention strategies that protect residents, staff, and communities for the long term.
Lyndon is the Managing Director of Infection Prevention Services (IPS), bringing over 30 years' experience supporting aged care providers across Australia and New Zealand.
With a background spanning outbreak response, compliance, and infection risk management — alongside hands-on experience leading teams, managing multi-site operations, and navigating business turnaround — he understands both the clinical and organisational pressures aged care providers face. Lyndon holds a Master of Commerce (Industrial Relations), and applies that foundation to the people, process, and growth challenges that come with running a complex healthcare services business.
He is passionate about building the systems and capability that make infection prevention sustainable — not just compliant — and about helping organisations grow their confidence alongside their practice.
Lyndon's focus is straightforward: strengthen operations, develop the right people, and drive proactive infection prevention strategies that protect residents, staff, and communities for the long term.
Erica Callaghan
Marketing Manager
Erica Callaghan is a dedicated professional with a rich background in agriculture and nutrient management. Growing up on her family's farm in Mid Canterbury, she developed a deep passion for farming. She currently resides on her partner's arable property in South Canterbury.
In 2017, Erica joined the Farm Sustainability team, focusing on nutrient management and environmental stewardship. In February 2024, she became the Manager of Marketing and Sales at Bug Control New Zealand - Infection Prevention Services, where her passion now includes improving infection prevention outcomes.
Outside of work, Erica loves cooking and traveling, often combining her culinary interests with her explorations in Italy and Vietnam. She enjoys entertaining family and friends and remains actively involved in farm activities, especially during harvest season.
Erica Callaghan is a dedicated professional with a rich background in agriculture and nutrient management. Growing up on her family's farm in Mid Canterbury, she developed a deep passion for farming. She currently resides on her partner's arable property in South Canterbury.
In 2017, Erica joined the Farm Sustainability team, focusing on nutrient management and environmental stewardship. In February 2024, she became the Manager of Marketing and Sales at Bug Control New Zealand - Infection Prevention Services, where her passion now includes improving infection prevention outcomes.
Outside of work, Erica loves cooking and traveling, often combining her culinary interests with her explorations in Italy and Vietnam. She enjoys entertaining family and friends and remains actively involved in farm activities, especially during harvest season.
Toni Sherriff
Clinical Nurse Specialist
Toni is a Registered Nurse with extensive experience in Infection Prevention and Control. Her career began as a kitchen hand and caregiver in Aged Care facilities, followed by earning a Bachelor of Nursing.
Toni has significant experience, having worked in Brisbane’s Infectious Diseases ward before returning home to New Zealand, where she continued her career as a Clinical Nurse Specialist in Infection Prevention and Control within Te Whatu Ora (Health NZ).
Toni brings her expertise and dedication to our team, which is instrumental in providing top-tier infection prevention solutions to our clients.
Toni is a Registered Nurse with extensive experience in Infection Prevention and Control. Her career began as a kitchen hand and caregiver in Aged Care facilities, followed by earning a Bachelor of Nursing.
Toni has significant experience, having worked in Brisbane’s Infectious Diseases ward before returning home to New Zealand, where she continued her career as a Clinical Nurse Specialist in Infection Prevention and Control within Te Whatu Ora (Health NZ).
Toni brings her expertise and dedication to our team, which is instrumental in providing top-tier infection prevention solutions to our clients.
Julie Hadfield
Accounts & Payroll
Julie is experienced in Accounts & Payroll Administration & after a long career in both the Financial & Local Government Sectors, is now working with our team. Julie brings her strong time management & organisational skills to our team, which is important to keep the company running in the background to enable the rest of our team to provide top notch service to all of our clients.
Julie is experienced in Accounts & Payroll Administration & after a long career in both the Financial & Local Government Sectors, is now working with our team. Julie brings her strong time management & organisational skills to our team, which is important to keep the company running in the background to enable the rest of our team to provide top notch service to all of our clients.
Andrea Murray
Content Editor
I attended Otago University in NZ and graduated as a Dental Surgeon. After 40 years in the profession, I retired in 2022. Infection prevention knowledge was part of everyday practice, dealing with sterilisation, hand hygiene, and cleaning.
Before retiring, I began doing some editing and proofreading for Bug Control as I am interested in the subject and in the English language. During the COVID-19 lockdown, I attended the ACIPC course "Introduction to Infection Prevention and Control", which increased my interest in the subject. I now work part-time as the Content Editor for the company.
I attended Otago University in NZ and graduated as a Dental Surgeon. After 40 years in the profession, I retired in 2022. Infection prevention knowledge was part of everyday practice, dealing with sterilisation, hand hygiene, and cleaning.
Before retiring, I began doing some editing and proofreading for Bug Control as I am interested in the subject and in the English language. During the COVID-19 lockdown, I attended the ACIPC course "Introduction to Infection Prevention and Control", which increased my interest in the subject. I now work part-time as the Content Editor for the company.
Personally, I lived in the UK for 10 years. My two children were born in Scotland, and now both are living in Europe, one in Amsterdam, Netherlands, and the other in Edinburgh, Scotland. I live close to Fairlie on the South Island of NZ, a beautiful part of the country, and I love being out of the city.
Princess
Customer Support
Princess began her career as a dedicated Customer Service Representative, honing her communication and problem-solving skills. She later transitioned into a Literary Specialist role, where she developed a keen eye for detail. Her journey then led her to a Sales Specialist position, where she excelled in client relations.
Now, as a Customer Support professional in Infection Prevention Services. Princess focuses on ensuring customer satisfaction, building loyalty, and enhancing the overall customer journey.
Princess began her career as a dedicated Customer Service Representative, honing her communication and problem-solving skills. She later transitioned into a Literary Specialist role, where she developed a keen eye for detail. Her journey then led her to a Sales Specialist position, where she excelled in client relations.
Now, as a Customer Support professional in Infection Prevention Services. Princess focuses on ensuring customer satisfaction, building loyalty, and enhancing the overall customer journey.
Dianne Newey
Senior Infection Prevention and Control Consultant
Dianne is a Senior Clinical Consultant at Infection Prevention Services (IPS), bringing over 35 years of nursing experience and a depth of clinical knowledge that most people would need two careers to accumulate.
Having served as Clinical Director at Royal Ryde Rehabilitation Hospital alongside a career spanning the full breadth of clinical practice, Dianne has seen it all — and more importantly, knows exactly what to do about it. She is the person in the room that everyone quietly hopes will speak first.
For more than seven years she has been a cornerstone of the IPS team, providing clinical advice, developing and reviewing policies and procedures, delivering monthly IPC webinars to IP Leads, and conducting environmental audits in aged care facilities across Australia and New Zealand. If infection prevention has a question, Dianne almost certainly has the answer — and she'll deliver it with a laugh that you'll hear from the other end of the corridor.
A true fountain of knowledge, wrapped in the kind of warmth and humour that only three decades of nursing can produce. Customers don't just trust Dianne — they look forward to hearing from her.
Dianne is a Senior Clinical Consultant at Infection Prevention Services (IPS), bringing over 35 years of nursing experience and a depth of clinical knowledge that most people would need two careers to accumulate.
Having served as Clinical Director at Royal Ryde Rehabilitation Hospital alongside a career spanning the full breadth of clinical practice, Dianne has seen it all — and more importantly, knows exactly what to do about it. She is the person in the room that everyone quietly hopes will speak first.
For more than seven years she has been a cornerstone of the IPS team, providing clinical advice, developing and reviewing policies and procedures, delivering monthly IPC webinars to IP Leads, and conducting environmental audits in aged care facilities across Australia and New Zealand. If infection prevention has a question, Dianne almost certainly has the answer — and she'll deliver it with a laugh that you'll hear from the other end of the corridor.
A true fountain of knowledge, wrapped in the kind of warmth and humour that only three decades of nursing can produce. Customers don't just trust Dianne — they look forward to hearing from her.
Caoimhe (Keva) Stewart
Clinical & Business Operations Manager
Caoimhe is the Clinical & Business Operations Manager at Infection Prevention Services (IPS), bringing a clinical background as a Registered Nurse across the UK and Australia — and an almost unsettling ability to make technology do exactly what she wants.
With experience in Occupational Health, Palliative Care, and Community Nursing, she understands the real challenges faced by healthcare teams. What she may lack in stature she more than makes up for in impact — Caoimhe is the kind of person who walks into a problem, sizes it up, and has three solutions before anyone else has finished reading the brief.
Customers love her. Not just because she delivers — though she always does — but because she genuinely cares about the outcome on the other side. She is passionate about creating seamless learning experiences and empowering organisations with the tools, knowledge, and support needed to strengthen infection prevention practices and improve care outcomes.
Small in size. Mighty in results. Completely irreplaceable.
Caoimhe is the Clinical & Business Operations Manager at Infection Prevention Services (IPS), bringing a clinical background as a Registered Nurse across the UK and Australia — and an almost unsettling ability to make technology do exactly what she wants.
With experience in Occupational Health, Palliative Care, and Community Nursing, she understands the real challenges faced by healthcare teams. What she may lack in stature she more than makes up for in impact — Caoimhe is the kind of person who walks into a problem, sizes it up, and has three solutions before anyone else has finished reading the brief.
Customers love her. Not just because she delivers — though she always does — but because she genuinely cares about the outcome on the other side. She is passionate about creating seamless learning experiences and empowering organisations with the tools, knowledge, and support needed to strengthen infection prevention practices and improve care outcomes.
Small in size. Mighty in results. Completely irreplaceable.
Bridgette Mackie
Clinical Nurse Educator
Bridgette is an experienced New Zealand Registered Nurse, qualified Healthcare Auditor, and Healthcare Educator with a strong background in clinical quality, competency assessment, and infection prevention. She has led large-scale OSCE and CAP training programmes for internationally qualified nurses, developed sector-specific educational resources, and coordinated HealthCERT audit preparation in the surgical sector.
Known for her engaging teaching style and genuine passion for supporting learners, Bridgette excels at making complex topics accessible and relevant. She blends operational leadership with a deep commitment to professional development and safe, effective practice.
Bridgette is an experienced New Zealand Registered Nurse, qualified Healthcare Auditor, and Healthcare Educator with a strong background in clinical quality, competency assessment, and infection prevention. She has led large-scale OSCE and CAP training programmes for internationally qualified nurses, developed sector-specific educational resources, and coordinated HealthCERT audit preparation in the surgical sector.
Known for her engaging teaching style and genuine passion for supporting learners, Bridgette excels at making complex topics accessible and relevant. She blends operational leadership with a deep commitment to professional development and safe, effective practice.