
May 8
Scabies in Aged Care: Recognition, Treatment, and Outbreak Management in Australia and New Zealand
What is Scabies, and why does it matter in Aged Care?
Scabies is a parasitic skin infestation caused by the microscopic mite Sarcoptes scabiei
var. hominis. The fertilised female burrows into the upper layer of the skin to lay eggs,
and the resulting hypersensitivity reaction produces the rash and itch recognised
clinically.
Scabies is spread through prolonged skin-to-skin contact - typically 15 to 20 minutes or
longer - and via shared bedding, towels, clothing, and upholstered furniture, where mites
can survive 24 to 36 hours off the host. In a residential aged care facility, close personal
care, shared linen, and high-touch communal spaces create conditions for rapid
transmission once a single case is missed.
Source: Scabies — CDNA National

Guidelines for Public Health Units (Communicable Diseases Network Australia).
A first infestation can take four to six weeks to produce symptoms; re-infestation may
produce symptoms within one to four days. That lag is why outbreaks are usually well
established before the index case is identified, and why proactive surveillance beats
reactive containment every time.
How does Scabies present in older residents?
In a younger adult, Scabies presents predictably: an itchy rash that worsens at night,
with burrows in the finger webs, wrists, axillae, and waistline. In your residents, the
picture is rarely that clear - recognising atypical presentations is the single most
important clinical message for your team.
Key differences in older people:
- Reduced or absent itch due to immunosenescence. Residents with cognitive impairment may also be unable to self-report.
- Atypical distribution. In bed-bound or mobility-impaired residents, the rash often appears on the back, buttocks, scalp, and the back of the ears.
- Misdiagnosis as eczema, dermatitis, drug reactions, xerosis, or “senile pruritus” - the most common reason outbreaks are not contained early.
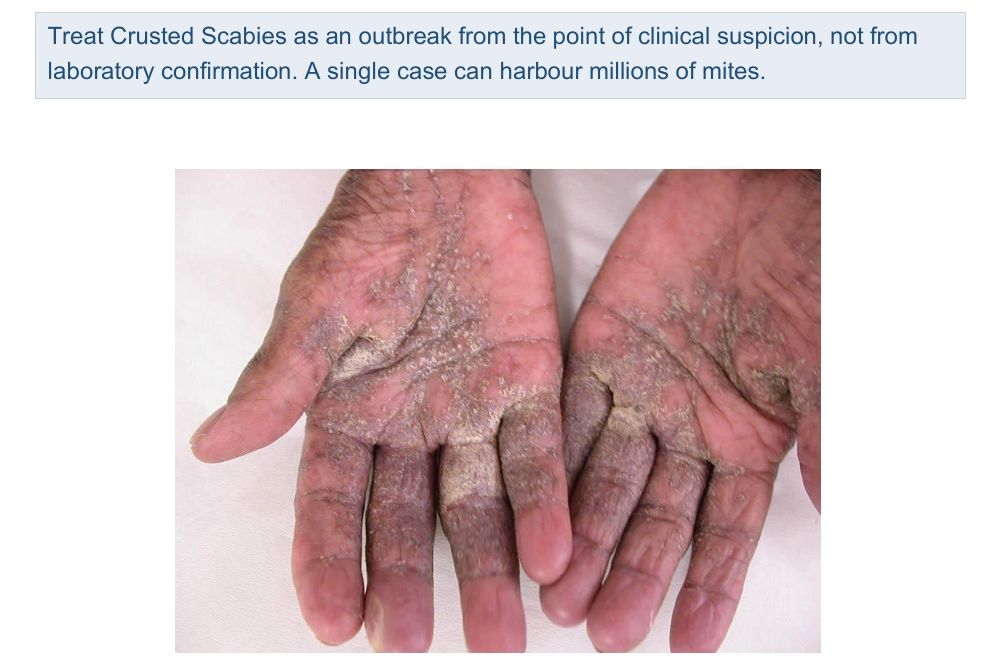
- Crusted Scabies presents as thick, hyperkeratotic plaques on the hands, feet,
elbows, or scalp, often without itching. Those at highest risk include residents with
advanced dementia, post-stroke immobility, long-term corticosteroid use, or end
stage frailty.
How is Scabies treated?
First-line treatment for classic Scabies is permethrin 5% cream, applied from the neck
down, including the scalp, hairline, behind the ears, and face (avoiding eyes and mouth)
in older or immunocompromised residents, left on overnight, then washed off in the
morning. The application is repeated on day seven to kill mites that hatch from eggs laid
after the first dose. Missing the second dose is the single most common reason for
treatment failure in aged care.
Oral ivermectin (200 micrograms/kg, repeated on days 7–14) is an alternative when topical application is impractical and is used in combination with permethrin for crusted scabies. Crusted Scabies also requires keratolytic agents to soften the crusts and specialist input from dermatology or infectious diseases.
Advise your team, residents, and families that post-scabietic itch can persist for two to four weeks after successful treatment. This is not a treatment failure. Manage it with emollients, antihistamines, and short courses of low-potency topical corticosteroids on a medical officer's order.
Oral ivermectin (200 micrograms/kg, repeated on days 7–14) is an alternative when topical application is impractical and is used in combination with permethrin for crusted scabies. Crusted Scabies also requires keratolytic agents to soften the crusts and specialist input from dermatology or infectious diseases.
Advise your team, residents, and families that post-scabietic itch can persist for two to four weeks after successful treatment. This is not a treatment failure. Manage it with emollients, antihistamines, and short courses of low-potency topical corticosteroids on a medical officer's order.
How do you manage an outbreak in your facility?
A Scabies outbreak is defined as two or more linked cases in time and place. Activate
your Outbreak Management Plan on a single confirmed case of Crusted Scabies, or on
two cases of classic Scabies within six weeks on the same wing or care team footprint.
Six workstreams must run in parallel - not sequentially:
- Confirm and notify. Notify your jurisdictional Public Health Unit (scabies is not nationally notifiable, but outbreaks in residential aged care require PHU involvement). Where the Serious Incident Response Scheme (SIRS) criteria are met, the Aged Care Quality and Safety Commission (ACQSC). In New Zealand, suspected or confirmed outbreaks in residential care must be notified to the local Medical Officer of Health / Public Health Unit under the Health Act framework.
- Contact tracing. Identify all close contacts from the previous six weeks - residents, care team, allied health, contractors, and visitors with prolonged contact.
- Mass treatment. Treat everyone on the affected wing on the same day, even if they are asymptomatic. Repeat on day seven. Record both doses in a treatment register.
- Isolation and PPE. Contact precautions until 24 hours after the first effective treatment (longer for crusted scabies). Long-sleeved gowns and gloves for direct care.
- Environmental decontamination. Hot wash (≥60°C) all bedding, towels, and clothing used in the past 72 hours. Bag and seal non-washables for 72 hours - 7 days for crusted scabies. Vacuum mattresses, upholstery, and carpets.
- Communication and documentation. Brief residents, families, and your full care
team. Maintain a line list, environmental cleaning logs, and notifications as evidence
of compliance with the Strengthened Aged Care Quality Standards and NZS
8134:2021 Ngā Paerewa.
Sources: Scabies — CDNA National Guidelines for Public Health Units (Communicable Diseases Network Australia);
Strengthened Aged Care Quality Standards (ACQSC); NZS 8134:2021 Ngā Paerewa (Standards New Zealand).

When is the outbreak over?
An outbreak is closed when no new cases have been identified for at least one full
incubation period (6 weeks) after the last treated case, and following Public Health Unit
agreement. Premature closure is one of the most consistent failure points in scabies
management because a quiet wing at week four can produce three new cases at week
five.
During the surveillance window, your IPC Lead should conduct weekly skin checks on the affected unit, monitor team members closely and retreat them at the first sign of recurrence, and audit environmental cleaning weekly. At week eight, debrief on the index case, the time from first symptom to diagnosis, and what your facility will change next time.
During the surveillance window, your IPC Lead should conduct weekly skin checks on the affected unit, monitor team members closely and retreat them at the first sign of recurrence, and audit environmental cleaning weekly. At week eight, debrief on the index case, the time from first symptom to diagnosis, and what your facility will change next time.
Take-Home Message
Scabies in aged care is rarely textbook. Routine skin assessment on admission and at
every clinical review detects scabies before it becomes an outbreak. And the difference
between treating one resident in week one and managing a wing-wide outbreak for two
months is built into your assessment templates, not your outbreak plan.
Follow our blogs on the HUB, IPS’s website. Ask EVE for an answer to the tricky
question or talk to our friendly team at support@infectioncontrol.care

Lyndon Forrest
Managing Director | CEO
Lyndon is the Managing Director of Infection Prevention Services (IPS), bringing over 30 years' experience supporting aged care providers across Australia and New Zealand.
With a background spanning outbreak response, compliance, and infection risk management — alongside hands-on experience leading teams, managing multi-site operations, and navigating business turnaround — he understands both the clinical and organisational pressures aged care providers face. Lyndon holds a Master of Commerce (Industrial Relations), and applies that foundation to the people, process, and growth challenges that come with running a complex healthcare services business.
He is passionate about building the systems and capability that make infection prevention sustainable — not just compliant — and about helping organisations grow their confidence alongside their practice.
Lyndon's focus is straightforward: strengthen operations, develop the right people, and drive proactive infection prevention strategies that protect residents, staff, and communities for the long term.
Lyndon is the Managing Director of Infection Prevention Services (IPS), bringing over 30 years' experience supporting aged care providers across Australia and New Zealand.
With a background spanning outbreak response, compliance, and infection risk management — alongside hands-on experience leading teams, managing multi-site operations, and navigating business turnaround — he understands both the clinical and organisational pressures aged care providers face. Lyndon holds a Master of Commerce (Industrial Relations), and applies that foundation to the people, process, and growth challenges that come with running a complex healthcare services business.
He is passionate about building the systems and capability that make infection prevention sustainable — not just compliant — and about helping organisations grow their confidence alongside their practice.
Lyndon's focus is straightforward: strengthen operations, develop the right people, and drive proactive infection prevention strategies that protect residents, staff, and communities for the long term.
Erica Callaghan
Marketing Manager
Erica Callaghan is a dedicated professional with a rich background in agriculture and nutrient management. Growing up on her family's farm in Mid Canterbury, she developed a deep passion for farming. She currently resides on her partner's arable property in South Canterbury.
In 2017, Erica joined the Farm Sustainability team, focusing on nutrient management and environmental stewardship. In February 2024, she became the Manager of Marketing and Sales at Bug Control New Zealand - Infection Prevention Services, where her passion now includes improving infection prevention outcomes.
Outside of work, Erica loves cooking and traveling, often combining her culinary interests with her explorations in Italy and Vietnam. She enjoys entertaining family and friends and remains actively involved in farm activities, especially during harvest season.
Erica Callaghan is a dedicated professional with a rich background in agriculture and nutrient management. Growing up on her family's farm in Mid Canterbury, she developed a deep passion for farming. She currently resides on her partner's arable property in South Canterbury.
In 2017, Erica joined the Farm Sustainability team, focusing on nutrient management and environmental stewardship. In February 2024, she became the Manager of Marketing and Sales at Bug Control New Zealand - Infection Prevention Services, where her passion now includes improving infection prevention outcomes.
Outside of work, Erica loves cooking and traveling, often combining her culinary interests with her explorations in Italy and Vietnam. She enjoys entertaining family and friends and remains actively involved in farm activities, especially during harvest season.
Toni Sherriff
Clinical Nurse Specialist
Toni is a Registered Nurse with extensive experience in Infection Prevention and Control. Her career began as a kitchen hand and caregiver in Aged Care facilities, followed by earning a Bachelor of Nursing.
Toni has significant experience, having worked in Brisbane’s Infectious Diseases ward before returning home to New Zealand, where she continued her career as a Clinical Nurse Specialist in Infection Prevention and Control within Te Whatu Ora (Health NZ).
Toni brings her expertise and dedication to our team, which is instrumental in providing top-tier infection prevention solutions to our clients.
Toni is a Registered Nurse with extensive experience in Infection Prevention and Control. Her career began as a kitchen hand and caregiver in Aged Care facilities, followed by earning a Bachelor of Nursing.
Toni has significant experience, having worked in Brisbane’s Infectious Diseases ward before returning home to New Zealand, where she continued her career as a Clinical Nurse Specialist in Infection Prevention and Control within Te Whatu Ora (Health NZ).
Toni brings her expertise and dedication to our team, which is instrumental in providing top-tier infection prevention solutions to our clients.
Julie Hadfield
Accounts & Payroll
Julie is experienced in Accounts & Payroll Administration & after a long career in both the Financial & Local Government Sectors, is now working with our team. Julie brings her strong time management & organisational skills to our team, which is important to keep the company running in the background to enable the rest of our team to provide top notch service to all of our clients.
Julie is experienced in Accounts & Payroll Administration & after a long career in both the Financial & Local Government Sectors, is now working with our team. Julie brings her strong time management & organisational skills to our team, which is important to keep the company running in the background to enable the rest of our team to provide top notch service to all of our clients.
Andrea Murray
Content Editor
I attended Otago University in NZ and graduated as a Dental Surgeon. After 40 years in the profession, I retired in 2022. Infection prevention knowledge was part of everyday practice, dealing with sterilisation, hand hygiene, and cleaning.
Before retiring, I began doing some editing and proofreading for Bug Control as I am interested in the subject and in the English language. During the COVID-19 lockdown, I attended the ACIPC course "Introduction to Infection Prevention and Control", which increased my interest in the subject. I now work part-time as the Content Editor for the company.
I attended Otago University in NZ and graduated as a Dental Surgeon. After 40 years in the profession, I retired in 2022. Infection prevention knowledge was part of everyday practice, dealing with sterilisation, hand hygiene, and cleaning.
Before retiring, I began doing some editing and proofreading for Bug Control as I am interested in the subject and in the English language. During the COVID-19 lockdown, I attended the ACIPC course "Introduction to Infection Prevention and Control", which increased my interest in the subject. I now work part-time as the Content Editor for the company.
Personally, I lived in the UK for 10 years. My two children were born in Scotland, and now both are living in Europe, one in Amsterdam, Netherlands, and the other in Edinburgh, Scotland. I live close to Fairlie on the South Island of NZ, a beautiful part of the country, and I love being out of the city.
Princess
Customer Support
Princess began her career as a dedicated Customer Service Representative, honing her communication and problem-solving skills. She later transitioned into a Literary Specialist role, where she developed a keen eye for detail. Her journey then led her to a Sales Specialist position, where she excelled in client relations.
Now, as a Customer Support professional in Infection Prevention Services. Princess focuses on ensuring customer satisfaction, building loyalty, and enhancing the overall customer journey.
Princess began her career as a dedicated Customer Service Representative, honing her communication and problem-solving skills. She later transitioned into a Literary Specialist role, where she developed a keen eye for detail. Her journey then led her to a Sales Specialist position, where she excelled in client relations.
Now, as a Customer Support professional in Infection Prevention Services. Princess focuses on ensuring customer satisfaction, building loyalty, and enhancing the overall customer journey.
Dianne Newey
Senior Infection Prevention and Control Consultant
Dianne is a Senior Clinical Consultant at Infection Prevention Services (IPS), bringing over 35 years of nursing experience and a depth of clinical knowledge that most people would need two careers to accumulate.
Having served as Clinical Director at Royal Ryde Rehabilitation Hospital alongside a career spanning the full breadth of clinical practice, Dianne has seen it all — and more importantly, knows exactly what to do about it. She is the person in the room that everyone quietly hopes will speak first.
For more than seven years she has been a cornerstone of the IPS team, providing clinical advice, developing and reviewing policies and procedures, delivering monthly IPC webinars to IP Leads, and conducting environmental audits in aged care facilities across Australia and New Zealand. If infection prevention has a question, Dianne almost certainly has the answer — and she'll deliver it with a laugh that you'll hear from the other end of the corridor.
A true fountain of knowledge, wrapped in the kind of warmth and humour that only three decades of nursing can produce. Customers don't just trust Dianne — they look forward to hearing from her.
Dianne is a Senior Clinical Consultant at Infection Prevention Services (IPS), bringing over 35 years of nursing experience and a depth of clinical knowledge that most people would need two careers to accumulate.
Having served as Clinical Director at Royal Ryde Rehabilitation Hospital alongside a career spanning the full breadth of clinical practice, Dianne has seen it all — and more importantly, knows exactly what to do about it. She is the person in the room that everyone quietly hopes will speak first.
For more than seven years she has been a cornerstone of the IPS team, providing clinical advice, developing and reviewing policies and procedures, delivering monthly IPC webinars to IP Leads, and conducting environmental audits in aged care facilities across Australia and New Zealand. If infection prevention has a question, Dianne almost certainly has the answer — and she'll deliver it with a laugh that you'll hear from the other end of the corridor.
A true fountain of knowledge, wrapped in the kind of warmth and humour that only three decades of nursing can produce. Customers don't just trust Dianne — they look forward to hearing from her.
Caoimhe (Keva) Stewart
Clinical & Business Operations Manager
Caoimhe is the Clinical & Business Operations Manager at Infection Prevention Services (IPS), bringing a clinical background as a Registered Nurse across the UK and Australia — and an almost unsettling ability to make technology do exactly what she wants.
With experience in Occupational Health, Palliative Care, and Community Nursing, she understands the real challenges faced by healthcare teams. What she may lack in stature she more than makes up for in impact — Caoimhe is the kind of person who walks into a problem, sizes it up, and has three solutions before anyone else has finished reading the brief.
Customers love her. Not just because she delivers — though she always does — but because she genuinely cares about the outcome on the other side. She is passionate about creating seamless learning experiences and empowering organisations with the tools, knowledge, and support needed to strengthen infection prevention practices and improve care outcomes.
Small in size. Mighty in results. Completely irreplaceable.
Caoimhe is the Clinical & Business Operations Manager at Infection Prevention Services (IPS), bringing a clinical background as a Registered Nurse across the UK and Australia — and an almost unsettling ability to make technology do exactly what she wants.
With experience in Occupational Health, Palliative Care, and Community Nursing, she understands the real challenges faced by healthcare teams. What she may lack in stature she more than makes up for in impact — Caoimhe is the kind of person who walks into a problem, sizes it up, and has three solutions before anyone else has finished reading the brief.
Customers love her. Not just because she delivers — though she always does — but because she genuinely cares about the outcome on the other side. She is passionate about creating seamless learning experiences and empowering organisations with the tools, knowledge, and support needed to strengthen infection prevention practices and improve care outcomes.
Small in size. Mighty in results. Completely irreplaceable.
Bridgette Mackie
Clinical Nurse Educator
Bridgette is an experienced New Zealand Registered Nurse, qualified Healthcare Auditor, and Healthcare Educator with a strong background in clinical quality, competency assessment, and infection prevention. She has led large-scale OSCE and CAP training programmes for internationally qualified nurses, developed sector-specific educational resources, and coordinated HealthCERT audit preparation in the surgical sector.
Known for her engaging teaching style and genuine passion for supporting learners, Bridgette excels at making complex topics accessible and relevant. She blends operational leadership with a deep commitment to professional development and safe, effective practice.
Bridgette is an experienced New Zealand Registered Nurse, qualified Healthcare Auditor, and Healthcare Educator with a strong background in clinical quality, competency assessment, and infection prevention. She has led large-scale OSCE and CAP training programmes for internationally qualified nurses, developed sector-specific educational resources, and coordinated HealthCERT audit preparation in the surgical sector.
Known for her engaging teaching style and genuine passion for supporting learners, Bridgette excels at making complex topics accessible and relevant. She blends operational leadership with a deep commitment to professional development and safe, effective practice.