
Feb 19
Tropical Pathogens: Dengue Fever in the Pacific
Considerations for HCWs in Aged Care
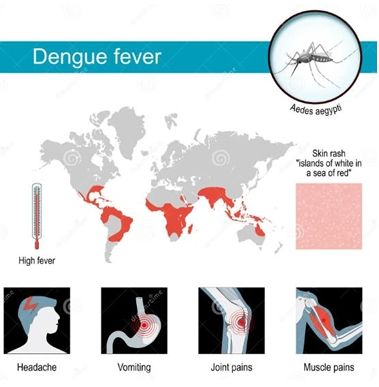
Dengue Fever is a tropical, mosquito-borne viral disease that is becoming more
prevalent in the Pacific region. Indeed, it is endemic in tropical Queensland, and with
climate change, is likely to impact other parts of Australasia wherever the Aedes
mosquito gains a foothold. Although not transmissible person-to-person, it has the
potential to infect others via an infected mosquito. Therefore, it is important to
recognise the disease and consider mosquito control in endemic regions as global
warming continues.
The possibility of the illness impacting aged care should be considered primarily due to staff travel, as an increasing number of healthcare workers are from tropical regions. HCWs can bring an infection back to their facility after visiting their home country. It is therefore worth considering dengue and other tropical diseases in aged care, not necessarily because of a direct risk, but of the possibility of the disease being introduced unknowingly. Person to person transmission, via Aedes mosquitoes in the immediate vicinity, could then be possible.
Facilities must then be able to distinguish a possible dengue infection from the flu and must avoid using aspirin or NSAIDs to prevent bleeding. Clinical vigilance, maintaining staff travel records, and ensuring adequate hydration are essential for safety.
The possibility of the illness impacting aged care should be considered primarily due to staff travel, as an increasing number of healthcare workers are from tropical regions. HCWs can bring an infection back to their facility after visiting their home country. It is therefore worth considering dengue and other tropical diseases in aged care, not necessarily because of a direct risk, but of the possibility of the disease being introduced unknowingly. Person to person transmission, via Aedes mosquitoes in the immediate vicinity, could then be possible.
Facilities must then be able to distinguish a possible dengue infection from the flu and must avoid using aspirin or NSAIDs to prevent bleeding. Clinical vigilance, maintaining staff travel records, and ensuring adequate hydration are essential for safety.

2025–2026 Dengue in the Pacific
The Pacific is currently under a "blue alert" for multiple Dengue strains (DENV-1 and
DENV-2).
- Cook Islands: Reporting over 600 cases as of February 2026, including the first dengue-related death of an older person with underlying conditions.
- Samoa: Confronting a prolonged epidemic with over 16,000 cases since early 2025.
- Other Regions: Intensified transmission is happening in French Polynesia and New Caledonia during the current hot and rainy season.
- Import Risk: New Zealand has already recorded over 80 "imported" cases, mainly linked to travel from the Cook Islands and Samoa.
- Dengue isn't spread from person to person, but through the bite of a mosquito
infected with the virus.
Why the Concern in Aged Care?
The interaction between a multicultural workforce and a highly vulnerable resident
population can put the aged care sector at risk of tropical illnesses, especially in
environments with local mosquito populations.
- Staff as "VFR" Travellers: Many staff members are "Visiting Friends and Relatives" (VFR) in high-risk areas such as the Philippines, India, Nepal, and the Pacific Islands.
- The "Silent" Entry: Staff may return to work during the 3-to-14-day incubation period or with mild symptoms, unaware they are carrying a pathogen.
- Resident Vulnerability: Some residents face a substantially increased risk of Severe Dengue (Dengue Haemorrhagic Fever).
- Comorbidities: In the older adults, high fever and dehydration can quickly
worsen existing conditions such as dementia or cardiovascular disease.
Identifying the Threat: Dengue vs. Influenza
Dengue is often called "breakbone fever" because of its severe pain, but in aged care, it
can be a "silent mimic".
- Sudden Onset: High fever often reaching 40°C (104°F).
- Pain Profile: Severe headache, particularly behind the eyes, along with muscle, joint, and bone pain.
- The Dengue Rash: A faint red rash or small purple spots usually appear 3–4 days after the fever begins.
- The Key Differentiator: If a resident has respiratory symptoms (cough/runny
nose), it is probably the Flu or COVID-19. If they lack respiratory symptoms but
have severe body aches and gastrointestinal symptoms, consider Dengue.
"Atypical" Signs in the Elderly
Nurses need to watch for subtle signs, as older adults might not always show a high
fever.
- The "Atypical" Slump: A sudden, unexplained decline in mobility, loss of appetite, or an unexpected fall.
- Bleeding Check: Look for abnormal bleeding from the gums during oral care or spontaneous bruising on the arms.
- The Critical Phase: The most dangerous time is paradoxically when the fever drops (Day 3–7). If the resident becomes restless, clammy, or experiences a drop in blood pressure, this is a medical emergency known as "Plasma Leakage".
Critical Treatment Protocols
There is no antiviral cure for Dengue; management is entirely supportive, but certain
medications are strictly prohibited.
- The "No Aspirin" Rule: Never use Aspirin or NSAIDs (Ibuprofen, Naproxen, Diclofenac). Because dengue affects blood clotting, these medications greatly increase the risk of severe internal bleeding.
- Hydration Priority: Prompt oral or IV fluid intake is essential to prevent dehydration, especially if there are gastrointestinal symptoms.
- Pain Management: Use only Paracetamol for fever and pain.
Beyond Dengue: Other Tropical Threats
Staff returning from international visits, VFR or recreational travel, may unintentionally
bring back other notifiable diseases.
- Measles: Highly contagious; can cause severe pneumonia in the elderly.
- Tuberculosis (TB): Latent TB can reactivate in communal living settings.
- Typhoid/Hepatitis A: Food-borne risks requiring strict enteric precautions in
kitchens.
Strategic Recommendations for Facility Managers
To safeguard residents and assist your team, think about these proactive measures:
- Travel Registry: Keep a record of staff returning from the Pacific, Southeast Asia, or South Asia.
- Non-Punitive Reporting: Promote a system where staff can report fevers or rashes within 21 days of returning without fear of losing income.
- Vector Control: Make sure all window screens are intact and remove any
standing water (for example, in flowerpots or gutters) to prevent local mosquito
populations from breeding.

- Clinical Vigilance: Flag any resident suspected of Dengue to immediately cease blood-thinning medications until cleared by a GP
Conclusion
In modern aged care settings, being "travel-aware" is crucial to providing high-quality
care. Protecting our residents is not about restricting the travel of our diverse workforce
but about fostering a culture of transparency and clinical awareness of tropical threats.
By recognising the subtle signs of Dengue, carefully managing medication protocols,
and vector control, we can ensure these challenges remain manageable risks rather
than turning into facility-wide crises.
See the HUB for more information from IPS.
We are on LinkedIn and Facebook – like, share and follow.
Can’t find what you’re looking for? Talk to EVE, our multilingual bot, or speak to someone real at support@infectioncontrol.care
Take advantage of our expertise in IPC. See the HUB for policies, resources and courses relating to this very important subject. Ask EVE for a quick answer to your question.
We are on LinkedIn and Facebook – like, share and follow.
Can’t find what you’re looking for? Talk to EVE, our multilingual bot, or speak to someone real at support@infectioncontrol.care
Take advantage of our expertise in IPC. See the HUB for policies, resources and courses relating to this very important subject. Ask EVE for a quick answer to your question.

Lyndon Forrest
Managing Director | CEO
Lyndon is the Managing Director of Infection Prevention Services (IPS), bringing over 30 years' experience supporting aged care providers across Australia and New Zealand.
With a background spanning outbreak response, compliance, and infection risk management — alongside hands-on experience leading teams, managing multi-site operations, and navigating business turnaround — he understands both the clinical and organisational pressures aged care providers face. Lyndon holds a Master of Commerce (Industrial Relations), and applies that foundation to the people, process, and growth challenges that come with running a complex healthcare services business.
He is passionate about building the systems and capability that make infection prevention sustainable — not just compliant — and about helping organisations grow their confidence alongside their practice.
Lyndon's focus is straightforward: strengthen operations, develop the right people, and drive proactive infection prevention strategies that protect residents, staff, and communities for the long term.
Lyndon is the Managing Director of Infection Prevention Services (IPS), bringing over 30 years' experience supporting aged care providers across Australia and New Zealand.
With a background spanning outbreak response, compliance, and infection risk management — alongside hands-on experience leading teams, managing multi-site operations, and navigating business turnaround — he understands both the clinical and organisational pressures aged care providers face. Lyndon holds a Master of Commerce (Industrial Relations), and applies that foundation to the people, process, and growth challenges that come with running a complex healthcare services business.
He is passionate about building the systems and capability that make infection prevention sustainable — not just compliant — and about helping organisations grow their confidence alongside their practice.
Lyndon's focus is straightforward: strengthen operations, develop the right people, and drive proactive infection prevention strategies that protect residents, staff, and communities for the long term.
Erica Callaghan
Marketing Manager
Erica Callaghan is a dedicated professional with a rich background in agriculture and nutrient management. Growing up on her family's farm in Mid Canterbury, she developed a deep passion for farming. She currently resides on her partner's arable property in South Canterbury.
In 2017, Erica joined the Farm Sustainability team, focusing on nutrient management and environmental stewardship. In February 2024, she became the Manager of Marketing and Sales at Bug Control New Zealand - Infection Prevention Services, where her passion now includes improving infection prevention outcomes.
Outside of work, Erica loves cooking and traveling, often combining her culinary interests with her explorations in Italy and Vietnam. She enjoys entertaining family and friends and remains actively involved in farm activities, especially during harvest season.
Erica Callaghan is a dedicated professional with a rich background in agriculture and nutrient management. Growing up on her family's farm in Mid Canterbury, she developed a deep passion for farming. She currently resides on her partner's arable property in South Canterbury.
In 2017, Erica joined the Farm Sustainability team, focusing on nutrient management and environmental stewardship. In February 2024, she became the Manager of Marketing and Sales at Bug Control New Zealand - Infection Prevention Services, where her passion now includes improving infection prevention outcomes.
Outside of work, Erica loves cooking and traveling, often combining her culinary interests with her explorations in Italy and Vietnam. She enjoys entertaining family and friends and remains actively involved in farm activities, especially during harvest season.
Toni Sherriff
Clinical Nurse Specialist
Toni is a Registered Nurse with extensive experience in Infection Prevention and Control. Her career began as a kitchen hand and caregiver in Aged Care facilities, followed by earning a Bachelor of Nursing.
Toni has significant experience, having worked in Brisbane’s Infectious Diseases ward before returning home to New Zealand, where she continued her career as a Clinical Nurse Specialist in Infection Prevention and Control within Te Whatu Ora (Health NZ).
Toni brings her expertise and dedication to our team, which is instrumental in providing top-tier infection prevention solutions to our clients.
Toni is a Registered Nurse with extensive experience in Infection Prevention and Control. Her career began as a kitchen hand and caregiver in Aged Care facilities, followed by earning a Bachelor of Nursing.
Toni has significant experience, having worked in Brisbane’s Infectious Diseases ward before returning home to New Zealand, where she continued her career as a Clinical Nurse Specialist in Infection Prevention and Control within Te Whatu Ora (Health NZ).
Toni brings her expertise and dedication to our team, which is instrumental in providing top-tier infection prevention solutions to our clients.
Julie Hadfield
Accounts & Payroll
Julie is experienced in Accounts & Payroll Administration & after a long career in both the Financial & Local Government Sectors, is now working with our team. Julie brings her strong time management & organisational skills to our team, which is important to keep the company running in the background to enable the rest of our team to provide top notch service to all of our clients.
Julie is experienced in Accounts & Payroll Administration & after a long career in both the Financial & Local Government Sectors, is now working with our team. Julie brings her strong time management & organisational skills to our team, which is important to keep the company running in the background to enable the rest of our team to provide top notch service to all of our clients.
Andrea Murray
Content Editor
I attended Otago University in NZ and graduated as a Dental Surgeon. After 40 years in the profession, I retired in 2022. Infection prevention knowledge was part of everyday practice, dealing with sterilisation, hand hygiene, and cleaning.
Before retiring, I began doing some editing and proofreading for Bug Control as I am interested in the subject and in the English language. During the COVID-19 lockdown, I attended the ACIPC course "Introduction to Infection Prevention and Control", which increased my interest in the subject. I now work part-time as the Content Editor for the company.
I attended Otago University in NZ and graduated as a Dental Surgeon. After 40 years in the profession, I retired in 2022. Infection prevention knowledge was part of everyday practice, dealing with sterilisation, hand hygiene, and cleaning.
Before retiring, I began doing some editing and proofreading for Bug Control as I am interested in the subject and in the English language. During the COVID-19 lockdown, I attended the ACIPC course "Introduction to Infection Prevention and Control", which increased my interest in the subject. I now work part-time as the Content Editor for the company.
Personally, I lived in the UK for 10 years. My two children were born in Scotland, and now both are living in Europe, one in Amsterdam, Netherlands, and the other in Edinburgh, Scotland. I live close to Fairlie on the South Island of NZ, a beautiful part of the country, and I love being out of the city.
Princess
Customer Support
Princess began her career as a dedicated Customer Service Representative, honing her communication and problem-solving skills. She later transitioned into a Literary Specialist role, where she developed a keen eye for detail. Her journey then led her to a Sales Specialist position, where she excelled in client relations.
Now, as a Customer Support professional in Infection Prevention Services. Princess focuses on ensuring customer satisfaction, building loyalty, and enhancing the overall customer journey.
Princess began her career as a dedicated Customer Service Representative, honing her communication and problem-solving skills. She later transitioned into a Literary Specialist role, where she developed a keen eye for detail. Her journey then led her to a Sales Specialist position, where she excelled in client relations.
Now, as a Customer Support professional in Infection Prevention Services. Princess focuses on ensuring customer satisfaction, building loyalty, and enhancing the overall customer journey.
Dianne Newey
Senior Infection Prevention and Control Consultant
Dianne is a Senior Clinical Consultant at Infection Prevention Services (IPS), bringing over 35 years of nursing experience and a depth of clinical knowledge that most people would need two careers to accumulate.
Having served as Clinical Director at Royal Ryde Rehabilitation Hospital alongside a career spanning the full breadth of clinical practice, Dianne has seen it all — and more importantly, knows exactly what to do about it. She is the person in the room that everyone quietly hopes will speak first.
For more than seven years she has been a cornerstone of the IPS team, providing clinical advice, developing and reviewing policies and procedures, delivering monthly IPC webinars to IP Leads, and conducting environmental audits in aged care facilities across Australia and New Zealand. If infection prevention has a question, Dianne almost certainly has the answer — and she'll deliver it with a laugh that you'll hear from the other end of the corridor.
A true fountain of knowledge, wrapped in the kind of warmth and humour that only three decades of nursing can produce. Customers don't just trust Dianne — they look forward to hearing from her.
Dianne is a Senior Clinical Consultant at Infection Prevention Services (IPS), bringing over 35 years of nursing experience and a depth of clinical knowledge that most people would need two careers to accumulate.
Having served as Clinical Director at Royal Ryde Rehabilitation Hospital alongside a career spanning the full breadth of clinical practice, Dianne has seen it all — and more importantly, knows exactly what to do about it. She is the person in the room that everyone quietly hopes will speak first.
For more than seven years she has been a cornerstone of the IPS team, providing clinical advice, developing and reviewing policies and procedures, delivering monthly IPC webinars to IP Leads, and conducting environmental audits in aged care facilities across Australia and New Zealand. If infection prevention has a question, Dianne almost certainly has the answer — and she'll deliver it with a laugh that you'll hear from the other end of the corridor.
A true fountain of knowledge, wrapped in the kind of warmth and humour that only three decades of nursing can produce. Customers don't just trust Dianne — they look forward to hearing from her.
Caoimhe (Keva) Stewart
Clinical & Business Operations Manager
Caoimhe is the Clinical & Business Operations Manager at Infection Prevention Services (IPS), bringing a clinical background as a Registered Nurse across the UK and Australia — and an almost unsettling ability to make technology do exactly what she wants.
With experience in Occupational Health, Palliative Care, and Community Nursing, she understands the real challenges faced by healthcare teams. What she may lack in stature she more than makes up for in impact — Caoimhe is the kind of person who walks into a problem, sizes it up, and has three solutions before anyone else has finished reading the brief.
Customers love her. Not just because she delivers — though she always does — but because she genuinely cares about the outcome on the other side. She is passionate about creating seamless learning experiences and empowering organisations with the tools, knowledge, and support needed to strengthen infection prevention practices and improve care outcomes.
Small in size. Mighty in results. Completely irreplaceable.
Caoimhe is the Clinical & Business Operations Manager at Infection Prevention Services (IPS), bringing a clinical background as a Registered Nurse across the UK and Australia — and an almost unsettling ability to make technology do exactly what she wants.
With experience in Occupational Health, Palliative Care, and Community Nursing, she understands the real challenges faced by healthcare teams. What she may lack in stature she more than makes up for in impact — Caoimhe is the kind of person who walks into a problem, sizes it up, and has three solutions before anyone else has finished reading the brief.
Customers love her. Not just because she delivers — though she always does — but because she genuinely cares about the outcome on the other side. She is passionate about creating seamless learning experiences and empowering organisations with the tools, knowledge, and support needed to strengthen infection prevention practices and improve care outcomes.
Small in size. Mighty in results. Completely irreplaceable.
Bridgette Mackie
Clinical Nurse Educator
Bridgette is an experienced New Zealand Registered Nurse, qualified Healthcare Auditor, and Healthcare Educator with a strong background in clinical quality, competency assessment, and infection prevention. She has led large-scale OSCE and CAP training programmes for internationally qualified nurses, developed sector-specific educational resources, and coordinated HealthCERT audit preparation in the surgical sector.
Known for her engaging teaching style and genuine passion for supporting learners, Bridgette excels at making complex topics accessible and relevant. She blends operational leadership with a deep commitment to professional development and safe, effective practice.
Bridgette is an experienced New Zealand Registered Nurse, qualified Healthcare Auditor, and Healthcare Educator with a strong background in clinical quality, competency assessment, and infection prevention. She has led large-scale OSCE and CAP training programmes for internationally qualified nurses, developed sector-specific educational resources, and coordinated HealthCERT audit preparation in the surgical sector.
Known for her engaging teaching style and genuine passion for supporting learners, Bridgette excels at making complex topics accessible and relevant. She blends operational leadership with a deep commitment to professional development and safe, effective practice.